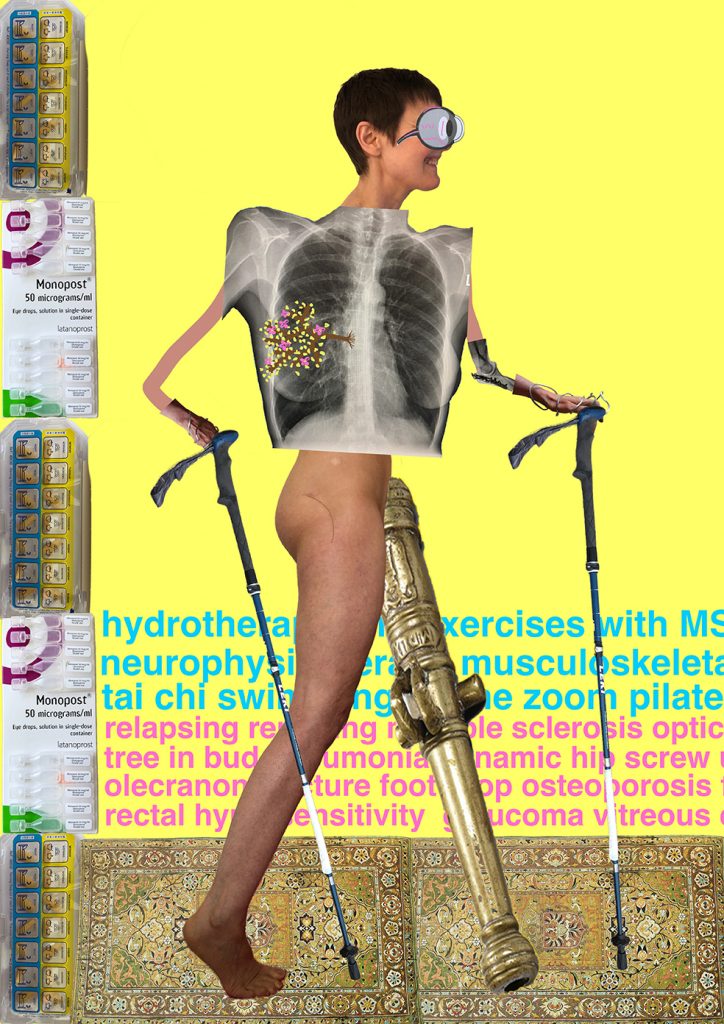
This self-portrait is a patients-eye view of Multimorbidity.
It’s a montage of my photos of me plus (some of) my x-rays.
With ageing populations worldwide, and the epidemiological transition towards long term conditions, multimorbidity is a huge and increasing problem. Long Covid is adding to this.
Although multiple diagnoses have multiplicative rather than simply additive effects, healthcare is still often taught and delivered as a series of single-specialty silos.
Our cost-effective expertise is rarely appreciated or built upon. We’re often not even respected: I’m showing my bottom – as ‘the system’ insists I do in those hospital ‘gowns’.
Like millions of multimorbid patients, I am much more than my diagnoses. I’m standing here on the iconic carpet I’m the world expert for.
In contrast, us patients and our families manage multiple conditions 24/7.
For those clinicians who persist in thinking of me solely as my diagnoses, I’ve included a pink (incomplete) list.
Im walking away from the medication (on the left). It doesn’t help much day-to-day.
Instead, with my stiff hands and leg-heavy-as-a-cannon, it’s exercise (in blue) that buoys me up. Now I’m unemployed, I’m struggling to pay for help with this. I’m waiting for a power wheelchair to get me out of the house – but dreading the electric bills.
It could be much worse: for example in a refugee camp or war zone.
But it could also be so much better: if services linked social and health care in real and practical ways; and especially when clinicians recognise that they can’t be a reliable barometer of what’s good for patients whose lived experiences, values, and goals deviate so substantially from theirs.
This image shows just one individual.